Smith & Nephew Porter's Five Forces Analysis
From Overview to Strategy Blueprint
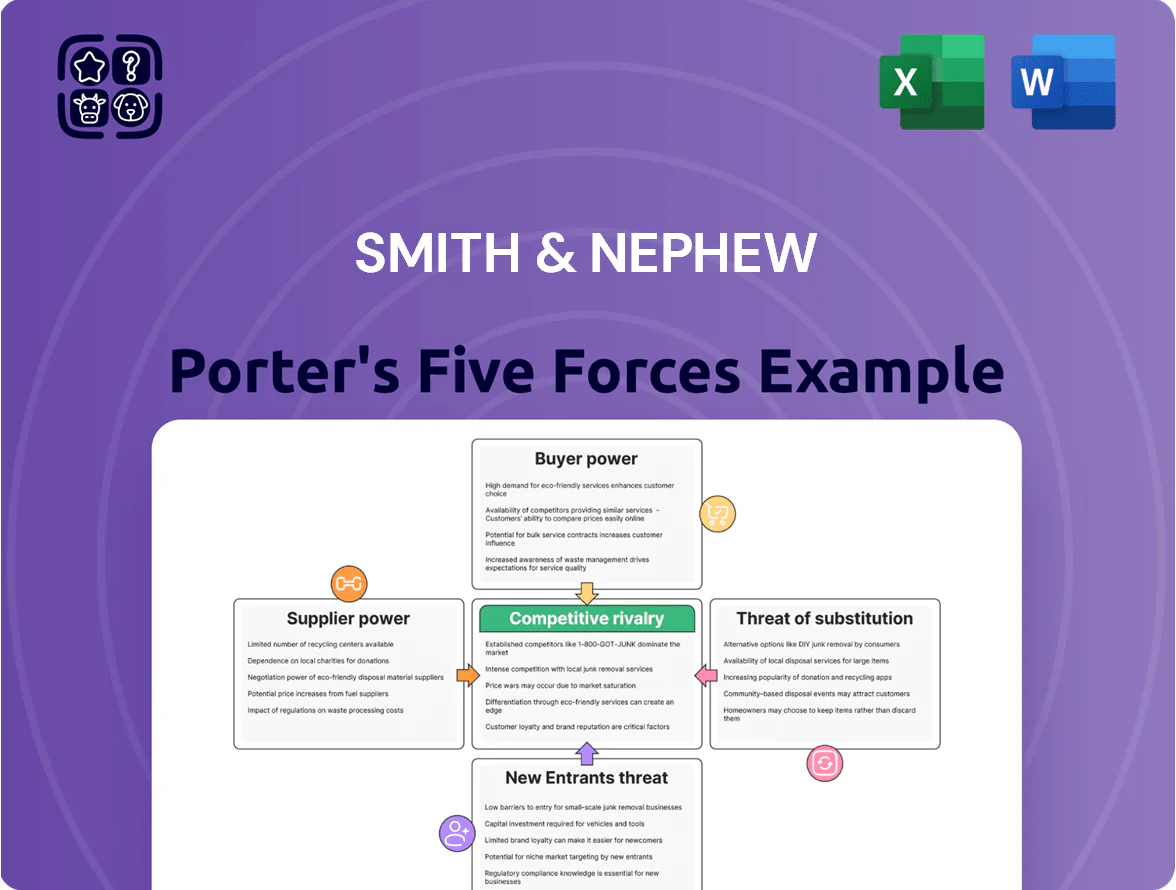
Smith & Nephew faces moderate competitive intensity: strong buyer bargaining from hospitals and value-based payment pressure, concentrated supplier power for specialized implants, high regulatory and IP barriers deterring new entrants, and growing substitute threats from non-surgical therapies and rivals’ innovations.
This brief snapshot only scratches the surface. Unlock the full Porter's Five Forces Analysis to explore Smith & Nephew’s competitive dynamics, market pressures, and strategic advantages in detail.
Suppliers Bargaining Power
Raw Material Commodity Price Volatility
Smith & Nephew depends on titanium, cobalt‑chrome and medical‑grade polymers for implants; these commodities saw price spikes in 2021–2024 (titanium up ~18% 2021–23, cobalt up ~35% 2020–22) that squeezed margins.
The firm uses multi‑year supply contracts and hedges; long‑term deals covered ~60% of metal needs in 2024, reducing volatility exposure but not eliminating higher purity cost risk.
Specialized Component Dependency
Certain advanced sensors and actuators for robotic-assisted surgery and digital tools come from few high-tech suppliers, giving them strong bargaining power; 2024 supplier concentration saw top-three vendors supplying ~65% of such modules industry-wide.
Their proprietary IP is embedded in Smith & Nephew designs, raising supplier leverage as alternatives require redesign.
Switching costs are high: regulatory re-certification (FDA 510(k) or PMA equivalents) typically adds 9–18 months and $1–5M in direct costs per device variant.

Strict Regulatory Compliance for Vendors
Suppliers in medtech must meet strict standards like ISO 13485 and FDA QSR; by 2025 about 68% of global medtech suppliers held ISO 13485 certification, shrinking the eligible partner pool for Smith & Nephew. Smaller firms often can’t bear compliance costs (certification + validation averages $120k–$500k upfront), so certified suppliers gain pricing leverage and faster contract access, raising supplier bargaining power.
Energy and Logistics Cost Pressures
Manufacturing and global distribution for Smith & Nephew face sustained cost pressure from volatile energy prices and shipping rates, which remained elevated through late 2025—global container freight rates averaged about 2,300 USD/FEU in 2025 Q4, up ~18% year-on-year, while industrial electricity prices in key markets rose 12–20% in 2025.
Logistics and energy suppliers have passed these increases down the chain, forcing Smith & Nephew to absorb margins or raise product prices; management reported 2025 supply-chain inflation added roughly 1.2 percentage points to COGS in FY2025.
Specialized handling for sterile medical devices limits rapid provider switches; certified cold-chain and sterile-chain carriers have high contracting frictions, extending provider transition timelines to 6–12 months and raising switching costs.
- Global container freight ~2,300 USD/FEU (2025 Q4)
- Industrial electricity +12–20% (2025)
- Supply-chain inflation ≈ +1.2 pp to COGS (FY2025)
- Provider switch lag 6–12 months due to sterile logistics
Labor Market Constraints for Skilled Manufacturing
Skilled production of precision orthopaedic instruments faces tight labor supply: global demand for CNC and biomedical technicians rose ~12% from 2019–2024, tightening talent pools across tech and medical firms.
Outsourced manufacturers use this scarcity to push contract rates up; industry reports showed subcontractor margins on precision machining climbed 150–300 basis points in 2024.
This human-capital constraint acts as indirect supplier power, raising Smith & Nephew’s COGS via higher outsourcing fees and wage pass-throughs.
- 12% rise in skilled demand (2019–2024)
- 150–300 bps margin lift for subcontractors in 2024
- Higher outsourcing rates → increased COGS for Smith & Nephew
Supplier power squeezes margins: input shocks, high recert costs, long lead times
Suppliers hold moderate‑to‑high power: concentrated high‑tech and certified raw‑material vendors, steep switching costs (9–18 months, $1–5M recert), and 2025 input shocks (container freight ~$2,300/FEU; industrial electricity +12–20%; supply‑chain inflation ≈+1.2 pp COGS) compress margins despite ~60% metals on long‑term contracts.
| Metric | Value |
|---|---|
| Metals on LTA (2024) | ~60% |
| Container freight (2025 Q4) | $2,300/FEU |
| Industrial electricity (2025) | +12–20% |
| Supply‑chain inflation to COGS (FY2025) | +1.2 pp |
| Switching recert time/cost | 9–18 months; $1–5M |
What is included in the product
Uncovers key drivers of competition, customer influence, and market entry risks tailored to Smith & Nephew, identifying disruptive threats, supplier/buyer power, and protective market dynamics to inform strategy and investor materials.
Concise Porter's Five Forces for Smith & Nephew—one-sheet view to spot competitive pressure, regulatory risks, supplier/buyer dynamics, and innovation threats for faster strategic decisions.
Customers Bargaining Power
Influence of Group Purchasing Organizations
In the US and major markets, Group Purchasing Organizations (GPOs) bundle buying for 1,000s of hospitals—Premier Inc. and Vizient alone cover ~50% of US acute-care spend—letting them extract discounts often 15–30% on implants and devices.
GPOs use that volume to demand rebates, prompt payment, and exclusivity, pressuring margins for medical device makers like Smith & Nephew (revenue £3.7bn in FY2024).
Smith & Nephew must keep key GPO contracts and clinical value data to stay on procurement lists and protect market share; losing one large GPO can cut access to tens of millions in annual hospital spend.
Consolidation of Hospital Systems
The wave of hospital M&A has created systems buying over 50% of US hospital volumes; centralized procurement teams use analytics to benchmark efficacy and price across suppliers, driving transparency—CMS data show system purchasing groups negotiated average discounts rising 8–12% from 2019–2023.
Smith & Nephew now faces concentrated buyer power: losing one health system can cut multi-year implant volumes by millions in revenue, so the company must prove clear cost-per-outcome advantages and RCT-backed clinical benefits to retain high-volume accounts.

Government Budget Constraints and Reimbursement
Publicly funded healthcare systems in Europe and key emerging markets faced austerity in 2025, with OECD reports showing median hospital budgets down 3–5% year-over-year; fixed reimbursement rates for hip and knee replacements (e.g., typical DRG payments €8,000–€12,000) cap pricing for Smith & Nephew.
When governments cut reimbursements, state buyers’ bargaining power rises, forcing price concessions or formulary exclusion; a 2024–25 EU survey found 42% of hospitals delayed premium implant purchases due to budget limits.
That shifts manufacturer competition from clinical performance to unit cost and supply efficiency; Smith & Nephew must reduce COGS or offer bundled-payment models to retain volume under shrinking margins.
Shift Toward Value Based Healthcare
Buyers push Smith & Nephew into value-based contracts where payment links to patient outcomes; global value-based care pilots grew 22% from 2020–2024, forcing risk-sharing on device makers.
Customers demand reimbursement for revisions within set windows, so hospitals require Smith & Nephew to cover revision costs or rebates, shifting margins and cash flow risk.
This trend makes buyers insist on bundled services: data analytics, outcomes tracking, clinician training, and extended warranties beyond the implant.
- 2024: ~30% of US health systems piloting outcome-based device deals
- Revisions covered typically 90–365 days
- Service bundles raise contract value 10–25%
Switching Costs and Surgeon Preference
Surgeons influence brand choice through training and preference, but hospitals now make final purchasing decisions—US hospitals centralized purchasing rose to ~68% of systems by 2023, cutting procurement costs and limiting niche product use.
This standardization shifts bargaining power to hospital finance teams; switching costs for hospitals fall as group contracts and GPOs (group purchasing organizations) secure discounts of 10–25%, reducing clinicians' leverage.
GPOs dominate U.S. acute spend, forcing Smith & Nephew into value-based, bundled deals
Buyers are highly concentrated: GPOs (Premier, Vizient) cover ~50% US acute spend, extracting 15–30% discounts; system purchasing rose to ~68% (2023). Smith & Nephew (revenue £3.7bn FY2024) faces price caps from DRGs (€8k–€12k) and austerity (OECD: hospital budgets −3–5% in 2025), driving value‑based deals (30% US systems piloting in 2024) and bundled-service demands.
| Metric | Value |
|---|---|
| GPO US share | ~50% |
| GPO discounts | 15–30% |
| Centralized purchasing | 68% (2023) |
| SN revenue | £3.7bn (FY2024) |
Preview Before You Purchase
Smith & Nephew Porter's Five Forces Analysis
This preview shows the exact Porter’s Five Forces analysis for Smith & Nephew you'll receive immediately after purchase—no surprises, no placeholders.
The document displayed here is the part of the full version you’ll get—fully formatted, ready for download and use the moment you buy.
You're looking at the actual, professionally written analysis; once you complete your purchase, you’ll get instant access to this precise file.

Product Information
Product Information
Shipping & Returns
Shipping & Returns
Description
From Overview to Strategy Blueprint
Smith & Nephew faces moderate competitive intensity: strong buyer bargaining from hospitals and value-based payment pressure, concentrated supplier power for specialized implants, high regulatory and IP barriers deterring new entrants, and growing substitute threats from non-surgical therapies and rivals’ innovations.
This brief snapshot only scratches the surface. Unlock the full Porter's Five Forces Analysis to explore Smith & Nephew’s competitive dynamics, market pressures, and strategic advantages in detail.
Suppliers Bargaining Power
Raw Material Commodity Price Volatility
Smith & Nephew depends on titanium, cobalt‑chrome and medical‑grade polymers for implants; these commodities saw price spikes in 2021–2024 (titanium up ~18% 2021–23, cobalt up ~35% 2020–22) that squeezed margins.
The firm uses multi‑year supply contracts and hedges; long‑term deals covered ~60% of metal needs in 2024, reducing volatility exposure but not eliminating higher purity cost risk.
Specialized Component Dependency
Certain advanced sensors and actuators for robotic-assisted surgery and digital tools come from few high-tech suppliers, giving them strong bargaining power; 2024 supplier concentration saw top-three vendors supplying ~65% of such modules industry-wide.
Their proprietary IP is embedded in Smith & Nephew designs, raising supplier leverage as alternatives require redesign.
Switching costs are high: regulatory re-certification (FDA 510(k) or PMA equivalents) typically adds 9–18 months and $1–5M in direct costs per device variant.
Strict Regulatory Compliance for Vendors
Suppliers in medtech must meet strict standards like ISO 13485 and FDA QSR; by 2025 about 68% of global medtech suppliers held ISO 13485 certification, shrinking the eligible partner pool for Smith & Nephew. Smaller firms often can’t bear compliance costs (certification + validation averages $120k–$500k upfront), so certified suppliers gain pricing leverage and faster contract access, raising supplier bargaining power.
Energy and Logistics Cost Pressures
Manufacturing and global distribution for Smith & Nephew face sustained cost pressure from volatile energy prices and shipping rates, which remained elevated through late 2025—global container freight rates averaged about 2,300 USD/FEU in 2025 Q4, up ~18% year-on-year, while industrial electricity prices in key markets rose 12–20% in 2025.
Logistics and energy suppliers have passed these increases down the chain, forcing Smith & Nephew to absorb margins or raise product prices; management reported 2025 supply-chain inflation added roughly 1.2 percentage points to COGS in FY2025.
Specialized handling for sterile medical devices limits rapid provider switches; certified cold-chain and sterile-chain carriers have high contracting frictions, extending provider transition timelines to 6–12 months and raising switching costs.
- Global container freight ~2,300 USD/FEU (2025 Q4)
- Industrial electricity +12–20% (2025)
- Supply-chain inflation ≈ +1.2 pp to COGS (FY2025)
- Provider switch lag 6–12 months due to sterile logistics
Labor Market Constraints for Skilled Manufacturing
Skilled production of precision orthopaedic instruments faces tight labor supply: global demand for CNC and biomedical technicians rose ~12% from 2019–2024, tightening talent pools across tech and medical firms.
Outsourced manufacturers use this scarcity to push contract rates up; industry reports showed subcontractor margins on precision machining climbed 150–300 basis points in 2024.
This human-capital constraint acts as indirect supplier power, raising Smith & Nephew’s COGS via higher outsourcing fees and wage pass-throughs.
- 12% rise in skilled demand (2019–2024)
- 150–300 bps margin lift for subcontractors in 2024
- Higher outsourcing rates → increased COGS for Smith & Nephew
Supplier power squeezes margins: input shocks, high recert costs, long lead times
Suppliers hold moderate‑to‑high power: concentrated high‑tech and certified raw‑material vendors, steep switching costs (9–18 months, $1–5M recert), and 2025 input shocks (container freight ~$2,300/FEU; industrial electricity +12–20%; supply‑chain inflation ≈+1.2 pp COGS) compress margins despite ~60% metals on long‑term contracts.
| Metric | Value |
|---|---|
| Metals on LTA (2024) | ~60% |
| Container freight (2025 Q4) | $2,300/FEU |
| Industrial electricity (2025) | +12–20% |
| Supply‑chain inflation to COGS (FY2025) | +1.2 pp |
| Switching recert time/cost | 9–18 months; $1–5M |
What is included in the product
Uncovers key drivers of competition, customer influence, and market entry risks tailored to Smith & Nephew, identifying disruptive threats, supplier/buyer power, and protective market dynamics to inform strategy and investor materials.
Concise Porter's Five Forces for Smith & Nephew—one-sheet view to spot competitive pressure, regulatory risks, supplier/buyer dynamics, and innovation threats for faster strategic decisions.
Customers Bargaining Power
Influence of Group Purchasing Organizations
In the US and major markets, Group Purchasing Organizations (GPOs) bundle buying for 1,000s of hospitals—Premier Inc. and Vizient alone cover ~50% of US acute-care spend—letting them extract discounts often 15–30% on implants and devices.
GPOs use that volume to demand rebates, prompt payment, and exclusivity, pressuring margins for medical device makers like Smith & Nephew (revenue £3.7bn in FY2024).
Smith & Nephew must keep key GPO contracts and clinical value data to stay on procurement lists and protect market share; losing one large GPO can cut access to tens of millions in annual hospital spend.
Consolidation of Hospital Systems
The wave of hospital M&A has created systems buying over 50% of US hospital volumes; centralized procurement teams use analytics to benchmark efficacy and price across suppliers, driving transparency—CMS data show system purchasing groups negotiated average discounts rising 8–12% from 2019–2023.
Smith & Nephew now faces concentrated buyer power: losing one health system can cut multi-year implant volumes by millions in revenue, so the company must prove clear cost-per-outcome advantages and RCT-backed clinical benefits to retain high-volume accounts.
Government Budget Constraints and Reimbursement
Publicly funded healthcare systems in Europe and key emerging markets faced austerity in 2025, with OECD reports showing median hospital budgets down 3–5% year-over-year; fixed reimbursement rates for hip and knee replacements (e.g., typical DRG payments €8,000–€12,000) cap pricing for Smith & Nephew.
When governments cut reimbursements, state buyers’ bargaining power rises, forcing price concessions or formulary exclusion; a 2024–25 EU survey found 42% of hospitals delayed premium implant purchases due to budget limits.
That shifts manufacturer competition from clinical performance to unit cost and supply efficiency; Smith & Nephew must reduce COGS or offer bundled-payment models to retain volume under shrinking margins.
Shift Toward Value Based Healthcare
Buyers push Smith & Nephew into value-based contracts where payment links to patient outcomes; global value-based care pilots grew 22% from 2020–2024, forcing risk-sharing on device makers.
Customers demand reimbursement for revisions within set windows, so hospitals require Smith & Nephew to cover revision costs or rebates, shifting margins and cash flow risk.
This trend makes buyers insist on bundled services: data analytics, outcomes tracking, clinician training, and extended warranties beyond the implant.
- 2024: ~30% of US health systems piloting outcome-based device deals
- Revisions covered typically 90–365 days
- Service bundles raise contract value 10–25%
Switching Costs and Surgeon Preference
Surgeons influence brand choice through training and preference, but hospitals now make final purchasing decisions—US hospitals centralized purchasing rose to ~68% of systems by 2023, cutting procurement costs and limiting niche product use.
This standardization shifts bargaining power to hospital finance teams; switching costs for hospitals fall as group contracts and GPOs (group purchasing organizations) secure discounts of 10–25%, reducing clinicians' leverage.
GPOs dominate U.S. acute spend, forcing Smith & Nephew into value-based, bundled deals
Buyers are highly concentrated: GPOs (Premier, Vizient) cover ~50% US acute spend, extracting 15–30% discounts; system purchasing rose to ~68% (2023). Smith & Nephew (revenue £3.7bn FY2024) faces price caps from DRGs (€8k–€12k) and austerity (OECD: hospital budgets −3–5% in 2025), driving value‑based deals (30% US systems piloting in 2024) and bundled-service demands.
| Metric | Value |
|---|---|
| GPO US share | ~50% |
| GPO discounts | 15–30% |
| Centralized purchasing | 68% (2023) |
| SN revenue | £3.7bn (FY2024) |
Preview Before You Purchase
Smith & Nephew Porter's Five Forces Analysis
This preview shows the exact Porter’s Five Forces analysis for Smith & Nephew you'll receive immediately after purchase—no surprises, no placeholders.
The document displayed here is the part of the full version you’ll get—fully formatted, ready for download and use the moment you buy.
You're looking at the actual, professionally written analysis; once you complete your purchase, you’ll get instant access to this precise file.